
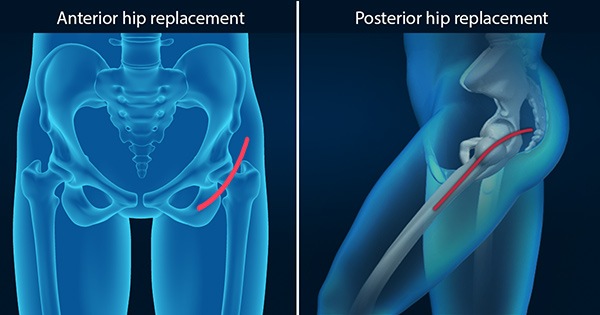
As a surgeon experienced with both anterior and posterior hip replacement surgery I get asked every week which approach is better. The answer is not as simple as you might think.
They main proposed benefit of the anterior approach is that it does not involve cutting any muscle, while the posterior approach does require a very small amount of muscle to be cut and repaired. In theory this could result in faster recovery and less risk of instability and dislocation (1). Recent evidence however does not support the promising early results of the anterior approach. Using modern enhanced recovery pathways there is no difference in early mobilisation and discharge between the anterior and posterior approaches (2). A 2019 study of 3574 patients also showed a lower rate of dislocations and overall complications with the posterior approach compared to the anterior approach (3). Another large study by the Adelaide based Australian Orthopaedic Association National Joint Replacement Registry looked at 5499 hips done by 68 surgeons and found that there is a significant learning curve with the anterior approach during which the rate of revision surgery is higher (4).
The potential problem with the anterior approach is that it is technically challenging and exposure of the femur (thigh bone) is more difficult compared to the posterior approach. This can result in component malposition, a fracture of the femur or other complications which are harder to recognise and deal with than when using other approaches. There are many hips for which the anterior approach is especially risky. There are particular anatomical variations of the hip bones that make exposure more difficult, as does obesity, and fracture is also more likely with older patients or those with osteoporosis.
It’s important to recognise that all hip replacement approaches have become less invasive over the years. The longer incisions and prolonged hospital stay of previous decades have given way to smaller incisions and rapid mobilisation for all patients regardless of surgical approach. Recent research also shows that with modern minimally invasive posterior approaches there is no need to restrict a patient’s activity after the surgery as we did in the past with the more invasive traditional posterior approach (5).
My view is that there is no advantage of the anterior approach over modern mini-posterior approaches. In my experience the anterior approach has a greater risk of serious complications and no advantage in terms of early walking and recovery compared to a mini posterior approach. My routine now is to use a mini posterior approach combined with an enhanced recovery after surgery pathway. Patients can stand and walk the same day as surgery, have no restrictions on movement after surgery and most can go home within one or two days. I am confident that this reduces the risk of complications and provides excellent short and long term outcomes for my patients.
For more information on hip replacement surgery click here:
If you would like to discuss hip replacement surgery with Dr Bauze then send us an email using the form on this page or call 81301259.
References
- Higgins BT, Barlow DR, Heagerty NE, Lin TJ. Anterior vs. posterior approach for total hip arthroplasty, a systematic review and meta-analysis. J Arthroplasty. 2015 Mar;30(3):419-34.
- Wainwright TW, Gill M, McDonald DA, Middleton RG, Reed M, Sahota O, Yates P, Ljungqvist O. Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Acta Orthop. 2020 Feb;91(1):3-19.
- Aggarwal VK, Elbuluk A, Dundon J, Herrero C, Hernandez C, Vigdorchik JM, Schwarzkopf R, Iorio R, Long WJ. Surgical approach significantly affects the complication rates associated with total hip arthroplasty. Bone Joint J. 2019 Jun;101-B(6):646-651.
- de Steiger RN, Lorimer M, Solomon M. What is the learning curve for the anterior approach for total hip arthroplasty? Clin Orthop Relat Res. 2015 Dec;473(12):3860-6.
- van der Weegen W, Kornuijt A, Das D. Do lifestyle restrictions and precautions prevent dislocation after total hip arthroplasty? A systematic review and meta-analysis of the literature. Clin Rehabil. 2016 Apr;30(4):329-39.





